
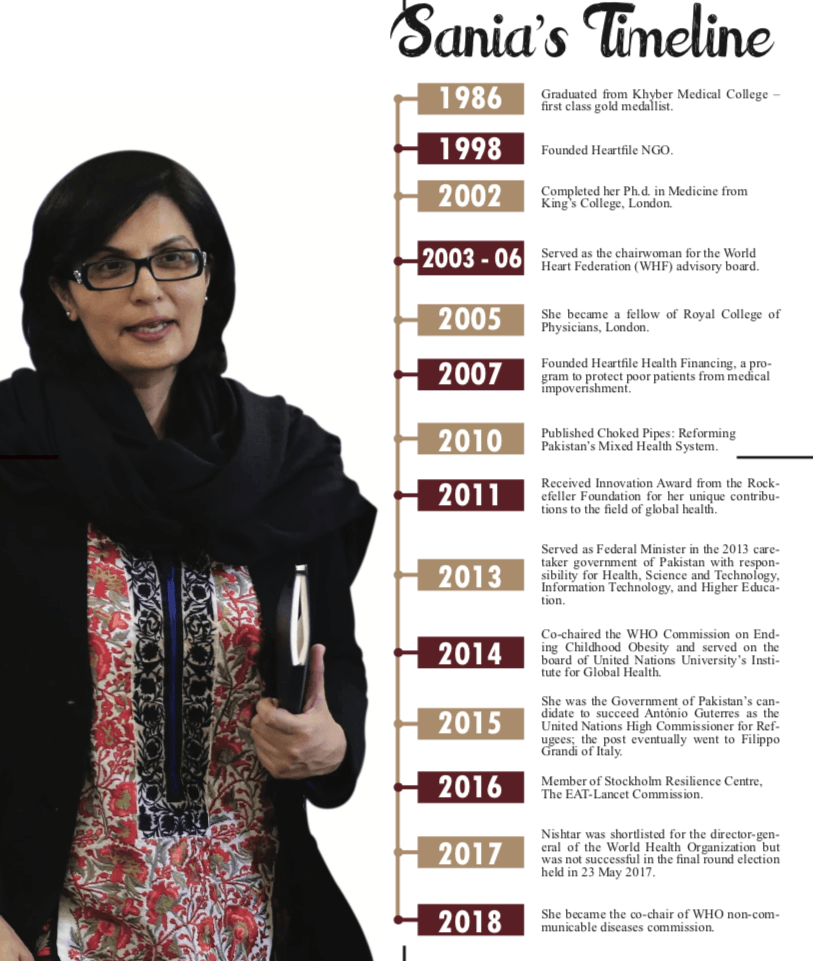
GVS sat down with Dr. Sania Nishtar, the internationally acclaimed health expert and the co-chair of WHO’s Commission on Non-Communicable Diseases. In the light of the World Health Day on April 6th, she shares future plans for Pakistan’s health sector.
GVS: We have seen your interest shift from health to governance over the years. Why is that the case?
Dr. Sania Nishtar: Anyone interested in improving the lives of the marginalized must realize that compassionate solutions and safety nets do not suffice. Lessons from around the developing world show that massive poverty reduction and quantum changes in the lives of the poor is the result of sustained economic growth and is dependent on consistent and effective policies, good governance and an overall environment where peace, security, law and order and justice attract investments.
In such settings, the trickle-down of economic development accrue benefits to people poor when economic freedoms extend to them and when an honest redistributive hand of the government, fosters competitiveness and impartial oversight as a counter against organized vested interests at various levels.
We, therefore, need deep-rooted governance reform to overcome systemic challenges. For example, improve revenue mobilization, systemic interventions in the labour market, reform of public finance management, procurement systems and civil service structures, overall transparency promoting measures, anti-corruption reform and effective systems of local governance. These impact all sectors including health. So, it is more worthwhile to aim for broader-based change.
Read more: Will ‘IoT’ technology revolutionize Pakistan’s healthcare
GVS: You have written much on health reform. What are Pakistan’s health challenges, where do they occur–villages, small town, tertiary–and why is this the case?
Dr. Sania Nishtar: When we examine challenges in the health sector, we take note of “manifestations”: overcrowded tertiary hospitals, under-utilized basic health units in villages, pervasive quackery, horrendous quality compromises, rising medical impoverishment, healthcare workers shortages, corruption and collusion in regulatory agencies, governance challenges, tenuous relationships between federal-provincial health agencies—I can go on and on.
Pakistan’s health system is beyond quick fixes. We need deep-rooted reform to overcome systemic challenges.
All these issues are manifestations, just as fever denotes infection and unexpected weather is indicative of climate change. We should get a better sense of the root causes. Unfortunately, the heath sector mirrors the overall state of governance. There are three core causes, which interact: inadequate state funding for the health sector, a burgeoning unregulated role of the private market in health, and lack of transparency in governance.
The state’s public health infrastructure has been chronically under-funded; its potential is eroded by rampant procurement collusion, crony deployments, and elite state capture. Market mechanisms have come into play to meet the ever-growing demand for healthcare, but in an environment of institutionalized regulatory rent-seeking and regulatory capture, the market—exceptions notwithstanding—doesn’t work for quality or equity. There are islands of progress both in the public and the private sector, but by and large, these sit in a sea of the underperforming health sector.
GVS: You have written extensively about solutions to this problem, your book Choked Pipes is a postgraduate textbook and your international publications on the subject are a reference. Can you summarize the solution in a nutshell?
Dr. Sania Nishtar: Pakistan’s health system is beyond quick fixes. We need deep-rooted reform to overcome systemic challenges. Foremost, we must recognize that broader reform of governance is critical to the success of reform within the health system and I have already talked about this in response to your earlier question.
Also, sustainable reform in the health sector, is dependent on institutional ability to conceptualize, implement, plough back learnings and refine reform on an ongoing basis. Sadly, in our country, there is an emphasis on politically visible quick initiatives without attention to the foundations on which reform must stand.
Foremost we must develop a national political consensus on a health reform agenda. Why can’t we have an all-party conference so that welfare reform can be insulated from the vacillations which are inherent to change in government? Increase public financing for health is critical and there are many ways to do that including labour market legislative changes. Pakistan’s health regulatory agencies are in need of reform but for that changes in laws/regulations are needed.
A number of ongoing ‘reform’ initiatives are underway by various provincial and federal governments, but what is key is to have the appropriate capacity within stewardship agencies (ministries/provincial departments) to examine which pilots and prototypes can be up-scaled in an evidence-based manner.
Read more: The only solution to america’s healthcare woes
GVS: Pakistan has a mix of both public and private health providers, and you have written extensively about the “mixed health systems syndrome” denoting the inefficiency that can arise when they co-exist. What can be the reform recipe?
Dr. Sania Nishtar: The public-private mix in health service delivery needn’t be a guarantee of poor performance. Public policy choices can be adapted to harness the potential of the private sector to achieve public sector goals. Some of these have been tested in Pakistan.
For example, the contracting out reform of basic health units was deployed at some scale from which many lessons can be drawn. However, far larger potential can be tapped if the state learns to draw on the outreach of privately practising doctors and enables them to deliver publicly financed essential services.
The ministry and provincial departments of health must develop stewardship mechanisms, to harness the potential of private healthcare providers. There is need for a fundamental rethink about the role of state in health and in other social services.
Financing, regulation and oversight are public responsibilities, but when it comes to the provision of services, the market can be organized to deliver on public goals. However, for that to happen, the public sector must re-engineer itself.
Read more: Pakistan’s ‘Tipping Point’
GVS: Many provincial governments are on the road to privatizing public hospitals. What do you think of that approach?
Dr. Sania Nishtar: Public hospitals, especially large tertiary care hospitals, their weaknesses notwithstanding are a safety net for the poor. These hospitals are under extreme pressure because of growing population needs and shrinking resources. The answer is not to divest from them but to address their capacity and performance constraints.
This is where collaboration with the private sector can offer solutions. Various options for public-private interaction/collaboration exist. These fall on a spectrum, at the extreme end of which is privatization and divestment of control, which is not recommended. The private sector can provide IT solutions and better management processes to improve performance. Many public-sector hospital functions can be outsourced.
Public ownership and not-for-profit service provision and autonomous governance arrangements offer some advantages over publicly financed, owned and operated models. However, evidence from international experiences shows that the gains in hospital autonomy are usually in the areas of revenues for hospitals and incentives for staff and to some level quality, but often at the cost of equity.
There is a need for specific safeguards in this respect in Pakistans setting. Also, when governments cannot afford to fund public hospitals, it appears logical to go for the public-private partnership model for developing healthcare infrastructure, which is being advocated for many developing countries.
Rise in foreign direct investments, business globalization, GATTS Agreements, opening up of markets and private investments in infrastructure can help in environments of shrinking or diminished public budgets. However, there are substantial costs associated with tendering for and negotiating public-private contracts. Governments must have the capacity for this purpose.
Read more: Pakistani origin Sajid Javid Britain’s new Interior Minister
GVS: After 18th Amendment, Pakistan’s health challenges have multiplied. Why is that? Issues exist over federal harmonization of food standards, drugs and regulatory issues on provincial levels.
Dr. Sania Nishtar: More broadly, major issues still lurk after passage of the 18th Amendment, which negatively impacts performance of the federal and provincial governments; for example, tensions over the mandate to regulate in devolved subjects, and federal government’s loss of constitutional mandate, to work for provincial equity and create a common union.
There are now three levels of “government” at the federal-provincial interface. The “federal government’s” mandates are outlined in the Federal Legislative List I (health information, global health), and the competent authority is the “cabinet”. The mandates of the “federation” are outlined in the Federal Legislative List II (regulation and training) and the competent authority here is the Council of Common Interests (though institutionally, the health ministry has to be responsible).
Every other health mandate is in the provincial domain. The mandates of the respective governments need to be clearly understood and respected. Most of the post-18th amendment issues arise due to lack of acceptance and respect for these boundaries.
GVS: When you were in the Caretaker Cabinet of 2013, you constituted the Ministry of Health. Can you explain why that was needed and how you were able to achieve that impossible target?
Dr. Sania Nishtar: The 18th amendment devolved 17 subjects and abolished corresponding ministries at the federal level. All decentralized federations have central ministries, responsible for certain functions, even for decentralized subjects. Dire consequences were envisaged with the health ministry’s abolition and resulting capacity fragmentation, especially in the face of pandemic threats.
Pakistan’s Constitution mandated the federal government to retain functions such as health information, but nobody was making a call for the re-establishment of the health ministry, given strong support for the 18th Amendment.
As a lone crusader, I campaigned for 2 years trying to make the case that there are central/national roles in federations for which we need a ministry of health. My writings, gained a lot of attention, (e.g, the paper Health and the 18th Amendment: Retaining National Roles in Devolution) and were being cited, both nationally and internationally.
I navigated a very difficult terrain to reestablish the ministry because I believed it was the right thing to do and because I feel that the job of the leader is precisely to get things done in a difficult situation.
All major international development partners could see the rationale for retaining some functions at the national level, but there was no action from the then government in terms of reinstalling the ministry of health. When I was inducted in the Caretaker Cabinet, I knew it was time to walk-the-talk and establish the ministry I had been campaigning for.
This was a difficult task, as there was a risk that it would be perceived as being opposed to the spirit of the popular 18th Amendment. I navigated a very difficult terrain to reestablish the ministry because I believed it was the right thing to do and because I feel that the job of the leader is precisely to get things done in a difficult situation.
The ministry’s creation was visibly successful. What stayed in the background was the multi-pronged coordinated effort I had to put behind the scene to enable its creation, garnering support from different levels, communicating with stakeholders, particularly the media and international community beforehand, and then navigating logistic details, after its creation to ensure transfer of assets and salaries so that the credibility of the initiative wouldn’t be in jeopardy due to mundane glitches. After its creation, I was deeply humbled by the congratulatory messages we received the day after from all over the world, including the head of WHO.
Read more: Is Imran Khan’s 11-points agenda really a roadmap for Naya Pakistan?
GVS: You chair the World Economic Forum’s Global Agenda Council on the future of healthcare, where there is increasing discussion about the role of technology in shaping the future of healthcare. Can you elaborate on the kind of opportunities technology is opening up?
Dr. Sania Nishtar: The future of health and healthcare is being shaped by many transformative forces. With billions of people connected with mobile devices, the combination of processing power, knowledge access and data portability can transform individual behaviours and disease management.
Artificial intelligence has the potential to overcome critical workers shortages, which consumed much of our health systems thinking in the last few decades. Blockchain can counter interoperability challenges in health IT systems and enable us to address clinical errors, wastage and fraud. Predictive analytics could reduce uncertainty in medicine.
Scalable business processes and interoperable solutions for exchanging patients’ information offer the potential to shape the future of service delivery. Use of easily deployable technology applications such as video surveillance can monitor Basic Health Units, just as fast food chains monitor their branches and GPS location technologies can be used to checkmate absenteeism in public service delivery.
Transformations are underway with Robotics, the Internet of things, 3D Printing, I can go on and on. We really have an opportunity to join dots, layer things up and reimagine a future for health—and that is what we are trying to do at the World Economic Forum.
But technology alone isn’t the solution. It has to be deployed in systems, with the right incentives structures. New governance and regulatory models are needed to set standards, formulate policy and address concerns around privacy and security which could hinder adoption. Partnerships are key to draw on the expertise of various sectors. Given these considerations, governments must invest in new capacities.
Read more: Why Pakistan’s first-ever Transgender School won’t be enough
GVS: You are the co-chair of the newly announced WHO Independent Global High-level Commission on NCDs. What are you doing in that role, why is this initiative important, and how do you think NCDs are impacting Pakistan?
Dr. Sania Nishtar: Non-communicable diseases, (which is a collective name for diabetes, cancers and heart and lung diseases) are the major global killers. They account for an annual estimated 38 million death toll and significant premature mortality. NCDs are not just the leading cause of death worldwide, but also pose a huge burden on societies and economies.
They are projected to incur economic losses of US$ 7 trillion over the next 15 years in case of inaction to address them. However, despite this evidence, NCDs were not in mainstream development planning and were even left out of the MDGs. This is one of the biggest public health paradoxes of our times.
The year 2018 is particularly important for NCDs as the United Nations General Assembly will host a summit on the subject, which is an unprecedented opportunity to address this challenge. The High-Level Global Commission on NCDs, has, therefore, being constituted to raise the profile of NCDs and to bring transformative recommendations to the table. I am honoured to be co-chairing this commission with three heads of state.
Read more: Losing a generation: The expense of malnutrition
GVS: Do you think World Health day has any significance in Pakistan? Are the celebrations productive and impactful enough to bring an improvement in the current health scenario of Pakistan?
Dr. Sania Nishtar: This year the theme of World Health Day centres on Universal Health Coverage (UHC), which is the central pillar in SDG 3, or the health SDG. UHC saves lives by promoting healthy life expectancy, reducing poverty, and protecting household incomes.
UHC is a nation’s promise to its people! According to worldwide surveys, health entitlements are amongst the most important entitlements citizens’ value. However, the success of UHC hinges on effective health systems. UHC can also enable achievement of disease-specific targets, the building of resilience against the health effects of climate change, and preventing and managing disease outbreaks.
With billions of people connected with mobile devices, the combination of processing power, knowledge access and data portability can transform individual behaviours and disease management.
There is a geographic access component to UHC, which means people shouldn’t have to travel long distances to access care. But there is also a financial access component to UHC, which means people should not become financially stressed, or forgo care or become impoverished in the process of seeking healthcare.
As you will appreciate, both of these challenges exist in Pakistan. Often, in remote settings and difficult terrains, people have to walk long distances to seek healthcare, and of course, you are aware of how serious the issue of medical impoverishment is. Geographic and financial access is not enough, we must also ensure that healthcare is safe and of quality.
Read more: Zardari aims to make Sindh a model province after winning 2018…
GVS: How do you see the quality of healthcare in the context of universal health coverage. We note that you also co-chair the United States National Academy of Sciences Global Study and the quality of healthcare. What is its relationship with Universal Health Coverage?
Dr. Sania Nishtar: Well, what good is healthcare if it is of poor quality or is harmful? Let’s take the matter of spurious drugs. Even if a poor person is able to access a health facility and has the means to pay for it or the state pays on his/her behalf a fake drug will nullify everything in the end and there are thousands of examples of poor quality.
GVS: Can you tell us a little bit about your work with Heartfile and how is this related to Heartfile Health Financing?
Dr. Sania Nishtar: Heartfile is the NGO think tank I have founded several years ago and most of its work is focused on policy research. Heartfile Health Financing is one of its flagship projects. At the humanitarian level, it provides financial access to treatment to those who are unable to pay.
As a leader, my philosophy has been not only to break that glass, but also to build a wide staircase so that others can follow.
Out of pockets payments force millions to spend catastrophically on healthcare or forego health care, altogether. This is one of the critical barriers to achieving Universal Health Coverage (UHC), which is one of the central pillars of Goal 3 of the sustainable development agenda.
It is well-known that financial access barriers impact women and girls in a poor household, most adversely. But there is a larger reform objective embedded in HHF, which is to supplement insurance and state funding to provide universal health coverage in mixed health systems. I hope to be able to upscale it globally.
Read more: Telenor partners with Inbox Technologies to improve agriculture
GVS: What do you think are the world’s biggest challenges? You hold key leading positions in the global health system. What do you think are the key health problems today, just as HIV and AIDs was a decade ago?
Dr. Sania Nishtar: Infectious outbreaks and emergencies with health consequences, antibiotic resistance (AMR) and the silent pandemic of Non-Communicable diseases (NCDs), are the biggest immediate threats to the collective health of people, worldwide.
These, together with the longer-term threat of climate change, threaten to wipe out the development gains of the last century. A flu pandemic in today’s inter-connected world could kill an estimated 80 million, even with the advanced medicines and technologies at hand.
Apart from pandemics, infectious outbreaks such as the Zika, can be devastating for societies and economies. Extreme climate events threaten the health and wellbeing of people across the world, particularly those in the Small Island Developing States.
Conflicts, disasters, and other catastrophes can lead to widespread public health emergencies. Health is one of the top concerns of the 130 million people who are affected by humanitarian crises across the globe, today.
GVS: Do you think enough is being done to bring/allow women to reach top leadership positions? How can we create a pipeline of women ready for top leadership positions? What institutional changes do we need in Pakistan?
Dr. Sania Nishtar: As is clear to so many of us, I understand that being a woman means you need to work twice as hard as the men, and perform to higher standards to get to a leadership position. In all areas of life and work there is a men’s club into which one cannot break – and women face a glass ceiling to make change– where they can see what needs to be done but there are no stairs for access.
As a leader, my philosophy has been not only to break that glass, but also to build a wide staircase so that others can follow. In terms of what can be done, firstly, it is important to mandate data disaggregation by gender across all information sources and unearth stories that averages tend to hide. We should give greater weightage to gender-related variables in composite measures.
Read more: Nine Pakistanis featured in Forbes Asia ‘30 Under 30’ list
Political parties should make election pledges to this effect and must be held accountable for delivery. Institutions should invest in mentoring, training opportunities, peer-to-peer learning and twinning, especially for women who could be potential leaders. I am committed to this agenda fully which is why I have agreed to join the advisory board of a new initiative called Global Health/5050.




")






